
Insomnia: Why You Can’t Sleep — and How to Actually Fix It
What Is Insomnia?
Insomnia disorder is defined as:
– Difficulty initiating sleep, maintaining sleep, or early morning awakening
– Occurring at least 3 nights per week
– For at least 3 months (chronic insomnia; under 3 months = acute insomnia)
– Despite adequate opportunity for sleep
– Causing significant daytime impairment
Chronic insomnia affects approximately 10–15% of adults and is more prevalent in women, older adults, and people with anxiety, depression, or chronic pain.
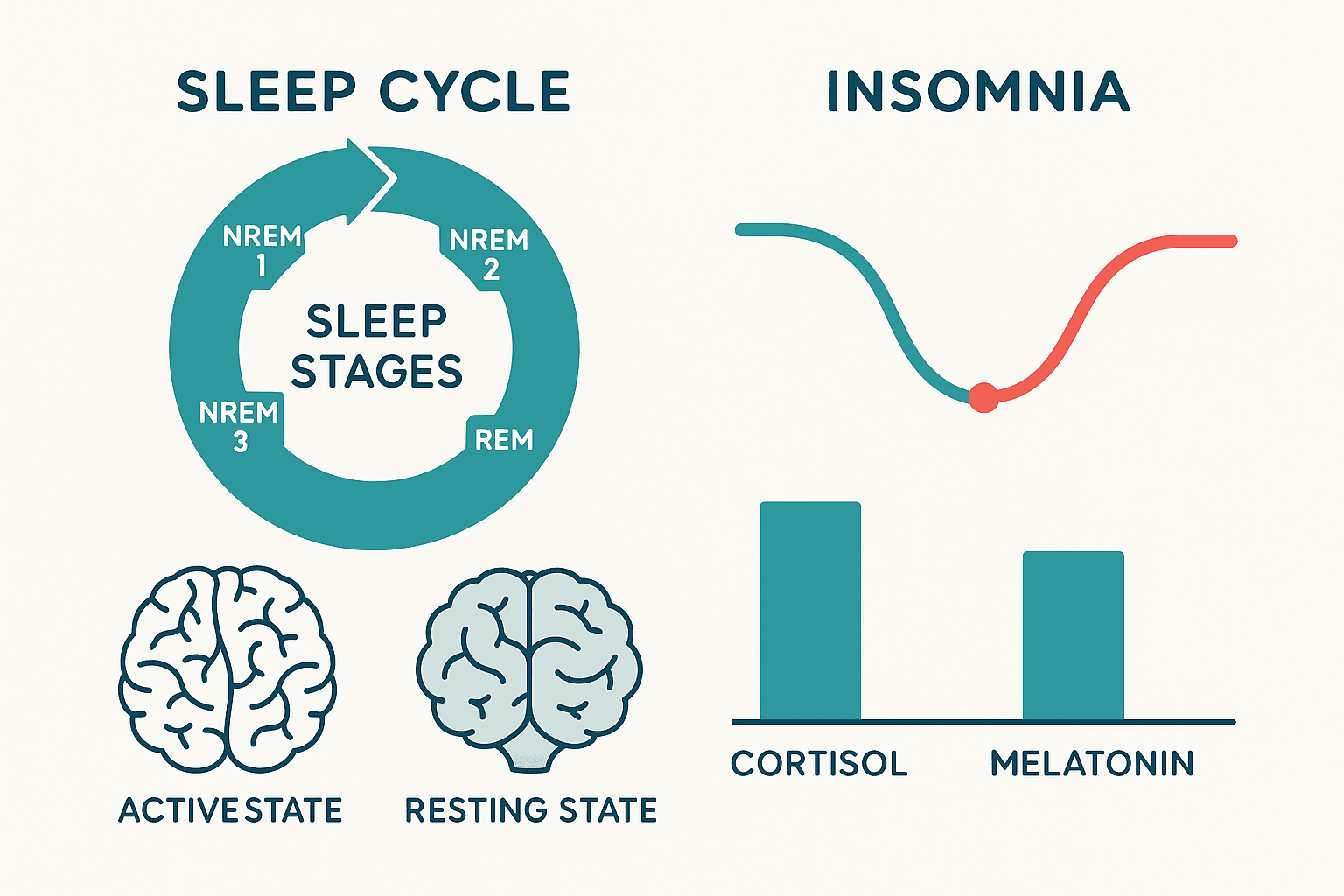
The Hyperarousal Model
The most evidence-supported model of chronic insomnia is hyperarousal — the sleep system is not broken, but the nervous system is in a state of elevated activation that prevents the transition to sleep. The hyperaroused insomniac:
- Has elevated cortisol, heart rate, and metabolic rate at night
- Has hyperactive amygdala and anterior cingulate cortex activity (the brain’s threat-monitoring regions)
- Has impaired prefrontal cortical quieting at sleep onset
- Has developed conditioned arousal — the bed and bedtime have become associated with alertness rather than sleep
This explains why behavioural interventions (CBT-I) are so effective — they directly address the conditioned and learned components of insomnia.
Common Contributors to Insomnia
- Anxiety and hyperarousal — the most common driver
- Depression — especially early morning awakening
- Hormonal changes — perimenopause and menopause are major triggers for sleep maintenance insomnia
- Cortisol dysregulation — elevated evening cortisol delays sleep onset; disrupted cortisol rhythm (e.g., flat curve from chronic stress) impairs sleep quality
- Poor sleep hygiene — irregular sleep times, screens before bed, caffeine, alcohol
- Medications — stimulants, steroids, SSRIs, beta-blockers, certain antihistamines
- Chronic pain — pain disrupts sleep; poor sleep amplifies pain (bidirectional)
- Sleep apnea — often misidentified as insomnia; snoring partner, morning headaches, daytime sleepiness are clues
- Circadian rhythm disruption — shift work, jet lag, irregular schedules
Self-Care for Insomnia
The Most Important Thing: Consistent Wake Time
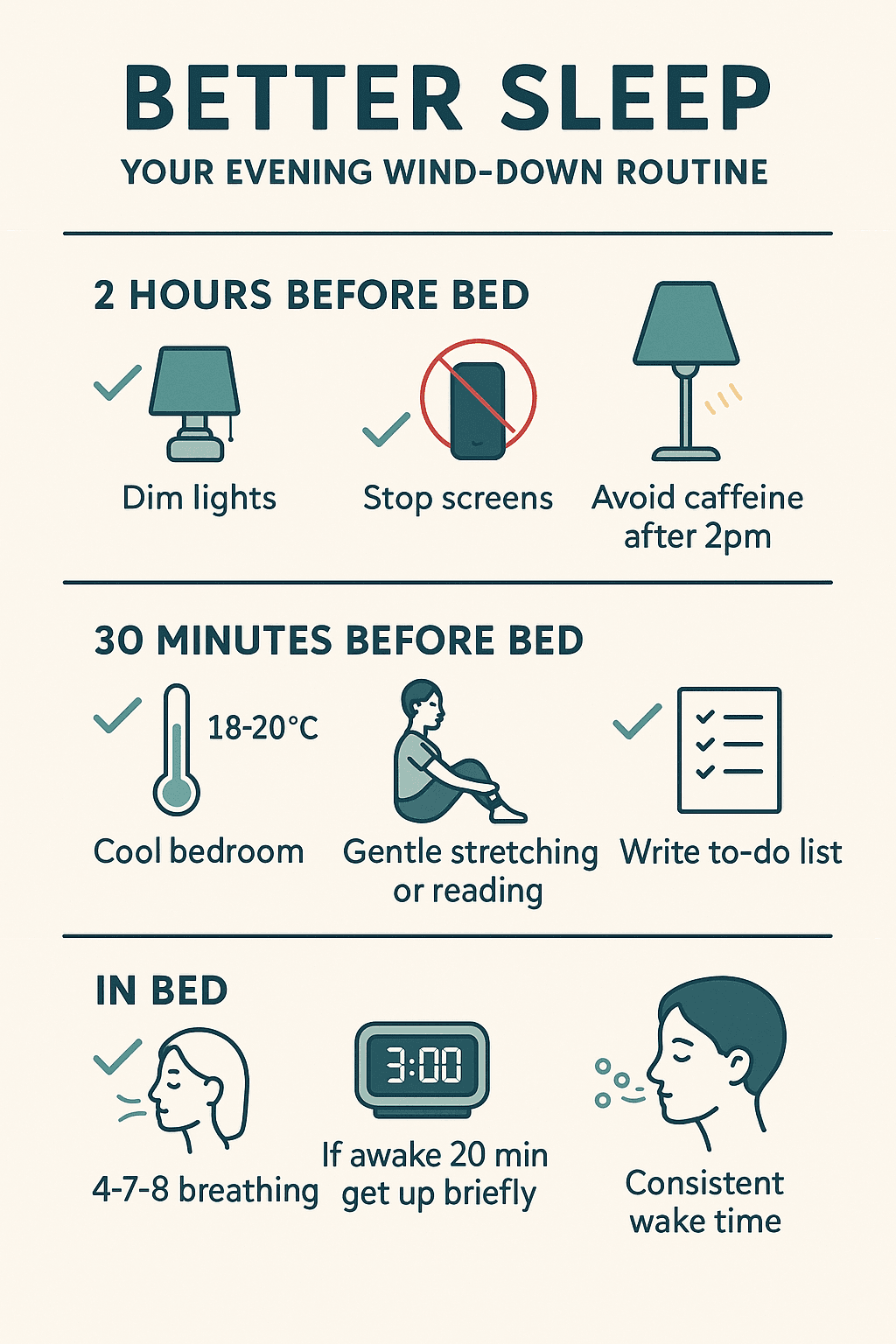
Set a consistent wake time 7 days a week — regardless of how poorly you slept. This is the single most powerful behavioural intervention for insomnia, because it anchors your circadian clock. Resist the temptation to sleep in after a bad night. The consolidation of sleep drive happens when your wake time is consistent.
Get Up When You Can’t Sleep
If you have been awake in bed for 20+ minutes, get up. Go to a dim, quiet room. Do something calm and non-stimulating. Return to bed only when sleepy. This breaks the conditioned association between the bed and wakefulness — the core of stimulus control therapy.
Light Exposure and Darkness
- Morning: 15–30 minutes of outdoor light within an hour of waking suppresses melatonin and anchors your sleep-wake cycle
- Evening: Dim lights 1–2 hours before bed; use blue-light-blocking glasses or software (f.lux) for screens; complete darkness for sleeping
Cool Bedroom
Core body temperature drops 1–2°C at sleep onset — facilitating the transition. Keep your bedroom at 16–19°C. A warm bath or shower 1–2 hours before bed causes the subsequent cooling that promotes sleep onset.
Caffeine Cutoff
Caffeine has a half-life of 5–7 hours. A cup of coffee at 2 PM still has half its caffeine at 7–9 PM. For people with insomnia, caffeine after noon is often problematic. Some people (slow metabolizers) are affected by morning coffee in the evening.
Reduce Alcohol
Alcohol induces sleep but fragments it severely in the second half of the night — suppressing REM sleep and causing rebound arousal. “It helps me sleep” is a common misperception; it helps you fall asleep but destroys sleep quality.
Frequently Asked Questions
Is melatonin safe for long-term use?
Short-term melatonin is safe and well-studied. Long-term use at the doses typically sold over the counter (5–10 mg) is less well-studied and may suppress endogenous melatonin production. Your naturopath will recommend the smallest effective dose, used for the shortest duration needed, and address the underlying causes of sleep disruption rather than relying on supplements indefinitely.
What about sleep medications?
Sedative-hypnotic medications (Z-drugs, benzodiazepines) are effective short-term but carry risks of dependence, tolerance, and rebound insomnia, and may impair memory and increase fall risk in older adults. CBT-I (cognitive-behavioural therapy for insomnia) is more effective than medication for long-term insomnia and should be considered before or alongside medication. Naturopathic treatment and acupuncture can be used alongside or as an alternative to medication.
I’ve had insomnia for years — can it really be fixed?
Yes — even long-standing insomnia responds to the right interventions. CBT-I has response rates of 70–80% for chronic insomnia. Identifying and addressing the specific biological contributors (cortisol, hormonal, nutritional) alongside behavioural change produces durable results for the majority of people.
For patient education only. Not medical advice.