Arthritis: Living Well and Moving More with Joint Pain
The Two Most Common Types
Osteoarthritis (OA)
Osteoarthritis is the most prevalent form — a degenerative condition in which the articular cartilage that cushions the ends of bones gradually breaks down. As cartilage wears, the bones begin to rub against each other, the joint space narrows, and the body responds by forming bone spurs (osteophytes) at joint margins. The synovial lining may also become inflamed.
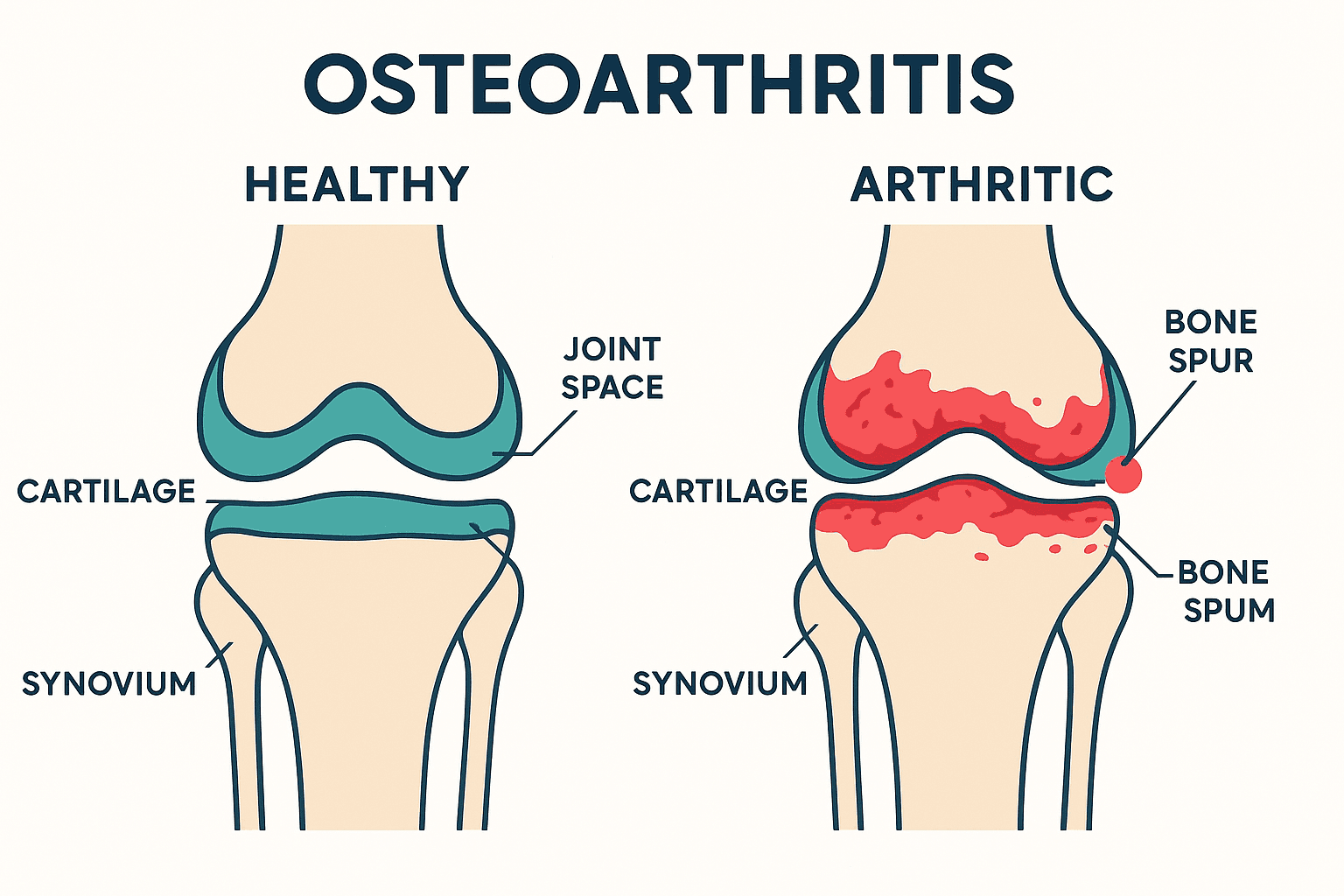
OA most commonly affects the knees, hips, hands, and spine. It is strongly associated with age (most common over 50), previous joint injury, excess body weight, and a lifetime of physical loading. Pain is typically activity-related — worse with use, better with rest — alongside morning stiffness that eases within 30 minutes.
Rheumatoid Arthritis (RA)
Rheumatoid arthritis is an autoimmune condition in which the immune system attacks the synovial lining of the joints, causing chronic inflammation, joint damage, and systemic symptoms. It typically affects the small joints of the hands and feet symmetrically, and produces morning stiffness lasting more than an hour, fatigue, and general unwellness. RA requires medical management (disease-modifying drugs) — physiotherapy plays an important complementary role.
Symptoms
Osteoarthritis
- Deep, aching joint pain that worsens with activity and improves with rest
- Morning stiffness lasting less than 30 minutes, and stiffness after prolonged inactivity (“gelling phenomenon”)
- Reduced range of motion — difficulty with activities requiring full joint movement
- Joint swelling — bony or soft tissue enlargement around the joint
- Crepitus — a creaking, grinding, or crackling sound and sensation with movement
- Joint instability in advanced cases
Rheumatoid Arthritis
- Symmetrical small joint involvement (fingers, wrists, toes)
- Morning stiffness lasting more than 1 hour
- Warmth, redness, and swelling in affected joints
- Fatigue and general malaise
- Possible extra-articular features (nodules, eye involvement, cardiovascular effects)
Living Well with Arthritis: Self-Care Strategies
Keep Moving
The single most important message in arthritis management: do not stop moving. Immobility accelerates joint stiffening, weakens supporting muscles, and reduces cartilage nutrition (which depends on the pumping action of movement to receive nutrients from synovial fluid). Low-impact activity — walking, swimming, cycling — is ideal.
Joint Protection Principles
- Avoid sustained joint loading in one position; change position regularly
- Use larger, stronger joints for tasks where possible (carry bags on your forearm, not your fingers)
- Pace activities — alternate demanding and restful tasks throughout the day
- Use assistive devices when appropriate (jar openers, ergonomic tools)
Heat and Cold
- Heat before activity to reduce stiffness and improve mobility
- Cold after activity or during flares to reduce swelling and pain
Water Exercise
Swimming, water walking, and aqua fitness are among the best exercise modes for arthritis — buoyancy reduces joint load by up to 90%, allowing free movement with minimal pain.
Weight Management
Even modest weight loss (5–10% of body weight) produces significant reductions in knee and hip OA pain. Your physiotherapist and naturopathic doctor can support this alongside a structured exercise plan.
Frequently Asked Questions
Does exercise make arthritis worse?
No — this is one of the most common and harmful misconceptions. Exercise improves OA outcomes at every stage. While it may cause temporary discomfort during the early weeks of a new program, the long-term benefits — reduced pain, improved function, slower progression — are unambiguous. Your physiotherapist will design a program appropriate for your current level.
Is arthritis hereditary?
Genetics plays a role in predisposing some people to arthritis — particularly RA and hand OA. However, lifestyle factors (activity level, weight, injury history) are equally or more important in determining whether and when arthritis develops and how severe it becomes.
Can arthritis be cured?
Currently, cartilage loss in OA cannot be reversed, and RA requires ongoing management. However, symptoms can be very significantly reduced, progression can be slowed, and most people with arthritis can maintain an active, independent life with appropriate treatment and self-management.
When should I consider joint replacement?
Joint replacement is typically considered when pain is severe, significantly limiting daily function, and has not responded to 6–12 months of conservative treatment. It is a very successful procedure for end-stage hip and knee OA, but the threshold for proceeding should account for your age, activity goals, and overall health.
For patient education only. Not medical advice.