
Perimenopause: What’s Happening in Your Body — and Why You Don’t Have to Just Cope
What Is Perimenopause?
Perimenopause is the transitional phase leading up to menopause — beginning when ovarian function starts to fluctuate and hormone levels become irregular, and ending 12 months after the final menstrual period (at which point menopause is officially reached).
It typically begins in the mid-to-late 40s (though for some women it starts in their late 30s) and lasts an average of 4–8 years — sometimes longer.
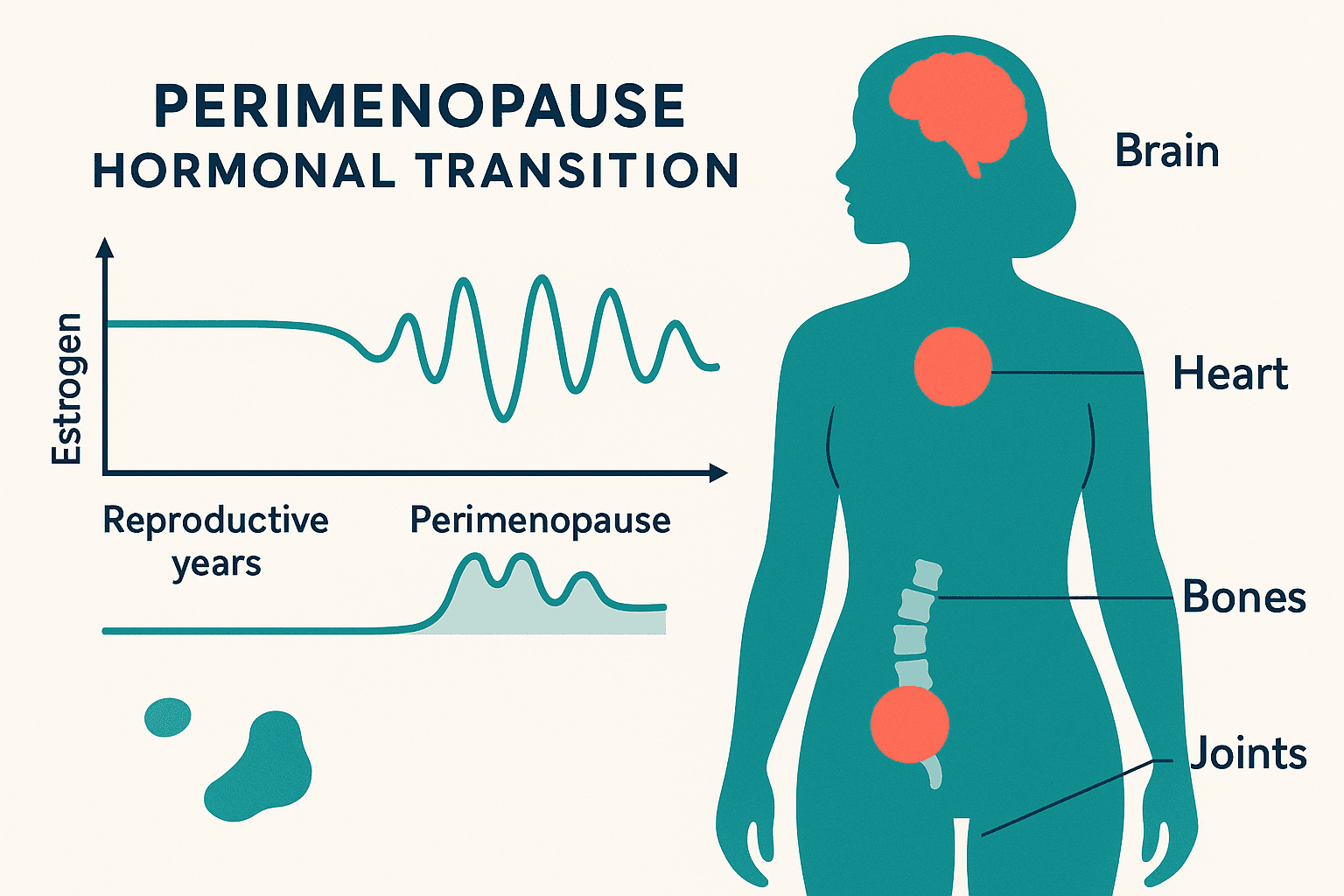
The hormonal hallmark of perimenopause is not simply declining estrogen, but wild fluctuation. Estrogen levels swing dramatically — sometimes very high, sometimes very low — before the overall trend downward. This erratic hormonal environment is responsible for many of the symptoms that are so confusing during the transition.
Progesterone typically declines earlier and more consistently than estrogen in perimenopause — this hormonal imbalance (estrogen relative dominance with low progesterone) contributes significantly to the heavy periods, sleep disruption, anxiety, and mood symptoms that often characterize early perimenopause.
Why Perimenopause Is Often Missed or Dismissed
Blood tests for FSH (follicle-stimulating hormone) are sometimes used to assess ovarian function, but during perimenopause FSH fluctuates dramatically — a single “normal” result does not rule out perimenopause. Many GPs are not trained to recognize perimenopause and may attribute symptoms to depression, anxiety, or stress.
If you are between 38–52 and experiencing the above symptoms — particularly in combination — perimenopause should be considered as the primary explanation.
Self-Care During Perimenopause
Track Your Cycle and Symptoms
A menstrual and symptom diary (or app like Clue, Flo, or Natural Cycles) reveals patterns that help your healthcare provider understand your hormonal picture — particularly the relationship between cycle phase and symptom severity.
Prioritize Sleep
Sleep disruption in perimenopause initiates and amplifies virtually every other symptom. Treat sleep as the priority treatment, not the symptom to manage around:
– Consistent bedtime and wake time
– Cool bedroom (16–18°C)
– Limit alcohol (disrupts sleep architecture and triggers hot flashes)
– Magnesium glycinate before bed
– Address anxiety — racing thoughts at 3 AM are often anxiety-driven and very responsive to naturopathic and acupuncture management
Exercise — But Smart
Exercise is strongly protective during perimenopause — reducing vasomotor symptoms, supporting bone density and muscle mass, improving mood, and managing metabolic changes. However, very high exercise loads (intensive endurance training, extreme caloric restriction) can worsen HPA axis dysregulation. Aim for: 150 min/week moderate cardiovascular activity + 2–3 sessions/week strength training.
Reduce Alcohol
Alcohol is a significant perimenopause aggravator — it disrupts sleep, triggers hot flashes, exacerbates mood symptoms, elevates breast cancer risk, and stresses the liver (which is processing your hormones). Even moderate drinking has noticeable effects on symptom severity during the transition.
Stress Management
The adrenal glands partially compensate for declining ovarian hormone production during perimenopause — but only when they are not already overwhelmed by chronic stress. Managing cortisol through consistent stress reduction practices (mindfulness, rest, boundary-setting, adaptogens) directly supports hormonal balance.
Your Perimenopause Deserves Attention
The perimenopausal transition is real, significant, and highly manageable with the right support. You don’t have to just cope. Book an appointment →
For patient education only. Not medical advice.