
Plantar Fasciitis: A Complete Guide to Understanding and Recovering from Heel Pain
That first step out of bed in the morning. You know the one. Your foot hits the floor and a sharp, searing pain shoots through your heel — so intense it makes you catch your breath and hobble to the bathroom like you’ve aged thirty years overnight.
If that sounds familiar, you’re far from alone. Plantar fasciitis is the most common cause of heel pain in adults, affecting between 4% and 7% of the general population at any given time. For runners it accounts for nearly 1 in 10 injuries. For people who spend long hours on their feet — nurses, teachers, retail workers, parents chasing toddlers — it can feel like a relentless, grinding companion that refuses to leave.
The good news: plantar fasciitis, while genuinely painful and frustrating, is highly treatable. Around 90% of people recover fully with the right conservative care. This guide will walk you through everything you need to know — what it is, why it happens, what actually works, and how to move forward with confidence.
What Plantar Fasciitis Actually Feels Like
Pain is deeply personal, and plantar fasciitis has a distinct character that most people describe in a consistent way:
- Sharp, stabbing heel pain — typically on the inner (medial) side of the heel, right where the arch meets the base of the foot
- Burning or shooting sensations that radiate into the arch
- A feeling of tightness along the bottom of the foot, as if a rubber band is pulled too tight
- Limping or toe-walking in the morning to avoid loading the heel
The most recognizable pattern is the morning pain spike: those agonizing first steps after getting out of bed, or after sitting at your desk for an hour and then standing up. This isn’t random — it has a specific cause (explained in the anatomy section below), and understanding it makes it far less frightening.
Many people also notice that the pain improves after they’ve been moving for 10–15 minutes, only to return if they stand or walk for extended periods. By the end of a long day on your feet, the heel often aches dully even at rest.
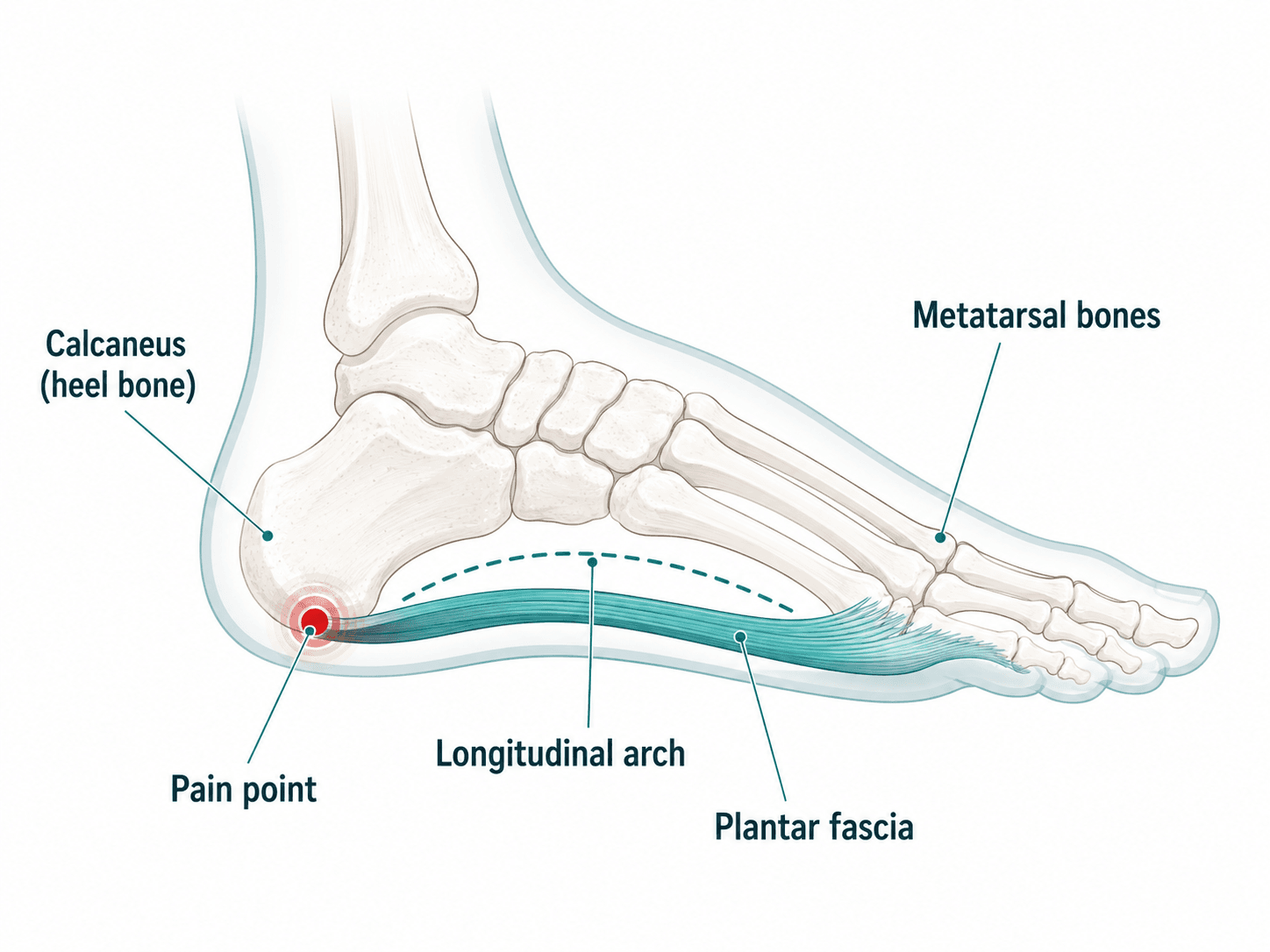
The Anatomy: What Is the Plantar Fascia?
To understand what’s happening in your foot, it helps to picture the structure involved.
The plantar fascia is a thick band of fibrous connective tissue — similar to a very dense ligament — that runs along the entire bottom of your foot. It originates at the calcaneal tuberosity (the medial tubercle of your heel bone) and fans out forward, splitting into five bands that attach to the base of each toe.
Think of it as the string of a bow: your foot is the bow, and the plantar fascia is the string that holds the arch in its curved shape. Without it, your arch would flatten under your body weight every time you take a step.
The fascia does remarkable work. During normal walking it absorbs up to 110% of your body weight with every step. During running, that jumps to 250%. It achieves this through what biomechanists call the windlass mechanism — when your toes bend upward during push-off, the fascia tightens around the heel like a winch, storing and releasing elastic energy and stabilizing the arch without requiring much muscle effort.
This is elegant engineering. But it also means the attachment point at your heel is under near-constant mechanical load — which is exactly where plantar fasciitis develops.
Why It’s Not Really “Inflammation”
Despite the “-itis” in its name (which implies inflammation), modern research has revealed that plantar fasciitis is not primarily an inflammatory condition. Tissue analysis consistently shows an absence of inflammatory cells — instead, what’s happening is collagen degeneration: the fibres of the fascia break down from repetitive mechanical overload, causing micro-tears that accumulate faster than the tissue can repair itself.
This is why the condition is increasingly called plantar fasciopathy or plantar fasciosis in clinical settings — a distinction explained in depth by Physiopedia’s clinical overview of plantar fasciitis — and it’s also why treatments that target inflammation (like cortisone injections) provide only short-term relief without addressing the underlying problem.
Why Does Plantar Fasciitis Develop?
Plantar fasciitis is what’s called an overuse injury — it develops gradually when the demand placed on the plantar fascia exceeds its capacity to recover. The tissue accumulates micro-damage faster than it can heal, and eventually that tipping point produces pain.
Several factors increase the load on the fascia or reduce its capacity to handle that load:
Biomechanical Factors
- Flat feet (pes planus): Increased strain at the fascia’s origin as the arch collapses under load
- High arches (pes cavus): Reduced shock absorption causes the fascia to take greater impact forces
- Excessive foot pronation or supination: Altered mechanics change how tension distributes through the fascia
- Reduced ankle dorsiflexion: Limited ankle mobility forces the foot into compensatory patterns that overload the heel
- Leg length discrepancy: Subtle differences in leg length alter gait and loading patterns
Muscle Tightness and Weakness
- Tight calf muscles (gastrocnemius and soleus) and a tight Achilles tendon are among the most consistent contributors — they restrict ankle movement and transfer force down into the fascia
- Weak intrinsic foot muscles leave the fascia to bear more of the arch-stabilizing work alone
Training and Lifestyle Factors
- Sudden increase in activity — starting a running program, dramatically increasing mileage, or a new job requiring prolonged standing
- Prolonged standing on hard surfaces without adequate footwear
- Inappropriate footwear — worn-out soles, minimal arch support, or shoes that hold the heel elevated and the toes extended for long periods
Who Is Most Affected?
Peak incidence is between 40 and 60 years of age, with women slightly more affected than men — particularly those aged 45–64, a period when hormonal changes associated with menopause may affect connective tissue resilience. It accounts for roughly 8% of all running injuries, and is common in active working adults and anyone whose occupation involves being on their feet for hours at a time. People with a higher BMI also carry greater mechanical risk, particularly those who are less athletically active.
Treatments at Wellness Place
The good news about plantar fasciitis is that it responds well to a combination of therapies, particularly when started before the condition becomes chronic. At Wellness Place we offer four treatments that have direct evidence for plantar heel pain — and for many patients, combining two or more produces faster, more lasting results than any single approach.
Physiotherapy
Physiotherapy is the cornerstone of plantar fasciitis treatment and is recommended as first-line care in clinical practice guidelines worldwide. Your physiotherapist at Wellness Place takes a whole-body view — the goal isn’t just to manage your heel pain, but to find and correct the underlying mechanics driving it.
A physiotherapy treatment plan typically includes:
Assessment and education: Understanding what’s causing your particular case — whether it’s calf tightness, arch biomechanics, training load, footwear, or a combination — is the foundation of effective treatment.
Manual therapy: Hands-on joint and soft tissue mobilization to improve mobility and reduce pain, including treatment of the calf, ankle, and foot itself.
High-load strength training: Research has consistently shown that progressive loading — not just rest — is what rebuilds the fascia’s capacity. A specific protocol involves unilateral heel raises performed with a towel rolled under the toes (to engage the windlass mechanism), which places the fascia under controlled load and stimulates tissue remodelling. Studies show this produces faster pain reduction than stretching alone. (See clinical evidence summary)
Taping: Low Dye taping reduces foot pronation and offloads the fascia insertion — particularly effective for short-term relief during the recovery period.
Orthotic prescription: Your physiotherapist can assess whether prefabricated or custom orthotics would help support your arch and cushion the heel during daily activity.
Plantar fascia-specific stretching: Targeted stretching protocol (detailed in the self-care section below) with instruction on timing and technique.
Around 90% of plantar fasciitis cases resolve successfully with conservative physiotherapy care within 12 months — often considerably sooner.
Shockwave Therapy
Shockwave therapy (formally: Extracorporeal Shockwave Therapy, or ESWT) is one of the most effective treatments available for stubborn plantar fasciitis — particularly in cases where the pain has persisted for three months or more and hasn’t responded fully to stretching and exercise alone.
The treatment uses high-energy acoustic waves delivered through a handheld device pressed against the heel. These pressure waves pass through the skin and reach the plantar fascia at the heel attachment. The biological effects include stimulating blood flow, promoting cellular repair, and — over a course of treatment — driving tissue remodelling in the degenerated fascia.
What the evidence shows: Three separate meta-analyses report ESWT has a success rate of over 60% for reducing heel pain — a finding supported by clinical reviews of shockwave therapy and outperforms placebo for pain reduction. It is also associated with fewer complications and faster return to normal activity compared to ultrasound or surgical interventions.
Most patients complete 3–5 sessions spaced one week apart. The treatment involves a brief period of discomfort during the session, but most people find it well-tolerated and notice progressive improvement between sessions.
Shockwave is particularly well-suited to Wellness Place because it pairs naturally with physiotherapy — your physio can address the mechanical causes while shockwave directly promotes healing in the damaged tissue.
Acupuncture
Traditional acupuncture and trigger point dry needling both have a role in plantar fasciitis, particularly for addressing the referred pain patterns and muscle tension that contribute to heel symptoms.
Trigger point dry needling of the gastrocnemius (calf) muscles is commonly used — taut bands and trigger points in the calf directly refer pain into the heel and arch, and releasing them reduces both the local symptoms and the mechanical strain on the fascia itself.
Acupuncture is considered a valuable option to try before moving to more invasive therapies. From a traditional acupuncture perspective, heel pain often relates to Kidney meridian points and local/adjacent points around the heel, ankle, and lower leg — a treatment approach that also addresses the systemic fatigue and stress that frequently accompany chronic pain conditions.
For patients whose plantar fasciitis is complicated by stress, poor sleep, or systemic inflammation, acupuncture’s broader regulatory effects can be a meaningful part of the overall recovery picture.
Massage Therapy (RMT)
Your Registered Massage Therapist plays a direct and practical role in plantar fasciitis recovery by working on the soft tissue components that physiotherapy and shockwave cannot fully address.
Key techniques include:
Deep friction massage of the plantar arch and heel insertion: Precisely applied friction breaks down adhesions in the degenerated fascia tissue and promotes healthier collagen remodelling.
Myofascial release of the foot: The plantar fascia is continuous with connective tissue throughout the foot and lower leg. Releasing the broader myofascial system — including the intrinsic foot muscles, the plantar surface, and surrounding structures — makes the foot more pliable and better able to absorb shock.
Calf and Achilles complex release: Given how central calf tightness is to plantar fasciitis, targeted work on the gastrocnemius, soleus, and Achilles tendon is a core part of every treatment. Reducing tension here directly reduces the pull on the heel insertion.
Manual soft tissue mobilization is strongly supported in clinical guidelines for plantar heel pain, and most patients notice meaningful relief in foot flexibility and heel tenderness after their first few sessions.
Recovery: What to Expect and How Long It Takes
Plantar fasciitis is a self-limiting condition with a strongly positive prognosis — meaning it will eventually get better. But “eventually” can feel discouraging when you’re dealing with it every single day.
Here is an honest recovery timeline:
| Timeframe | What Typically Happens |
|---|---|
| Weeks 1–4 | Reduction in morning pain severity; improved mobility with consistent stretching and load management |
| Weeks 4–8 | Noticeable improvement in daily pain levels; able to walk longer distances without significant discomfort |
| Months 2–4 | Progressive return to full activity; strengthening exercises increase fascia capacity |
| Months 4–12 | Full resolution for the majority of patients with consistent treatment |
A few important things to understand about recovery:
It is not linear. You will have good days and flare days. A flare after a long day or a change in footwear is not a setback — it’s normal tissue behaviour during healing. Judge progress over weeks, not days.
Rest alone is not enough. Passive rest removes the pain stimulus temporarily but does nothing to rebuild the fascia’s capacity. Active rehabilitation — particularly progressive loading exercises — is what produces lasting recovery.
Early treatment = faster recovery. The longer plantar fasciitis goes untreated, the more ingrained the tissue changes become. If you’ve been limping through it for six months, recovery will take longer than if you start treatment at week four. It’s never too late, but earlier is always better.
Self-Care Strategies You Can Start Today
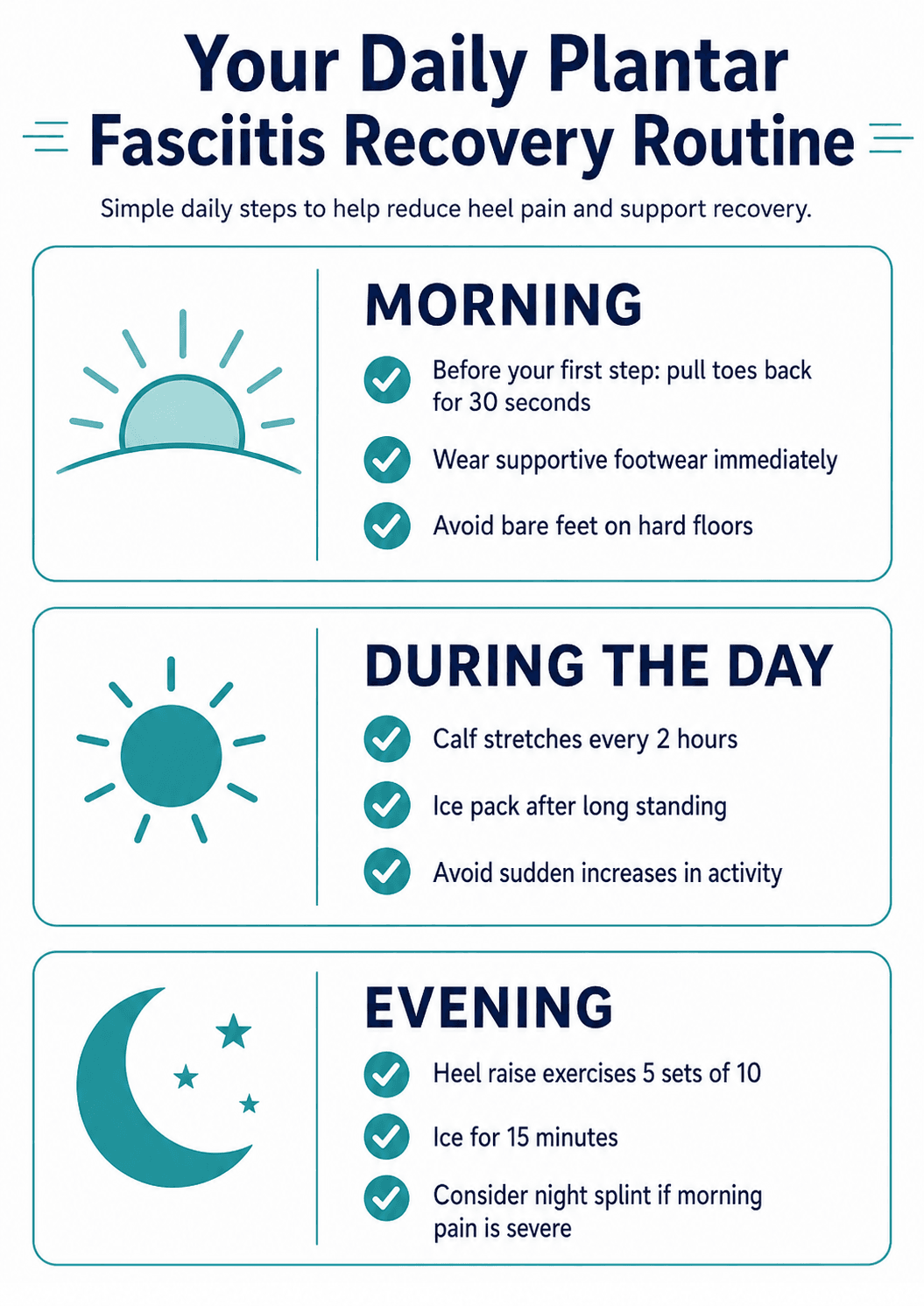
These evidence-based strategies are safe to begin immediately and have a meaningful impact on recovery, particularly when used alongside professional treatment.
The Essential Morning Stretch (Do This Before Your First Step)
This is the single most impactful self-care habit for plantar fasciitis.
Before getting out of bed:
1. Sit up and cross the affected foot over your opposite knee
2. Use your fingers to pull your toes back toward your shin until you feel a stretch along the arch
3. Hold for 30 seconds; repeat 3 times
4. Only then place your foot on the floor
This warms up the fascia from its overnight-shortened position and dramatically reduces that first-step pain. Doing the same stretch after any period of prolonged sitting also helps.
Calf and Achilles Stretching
Gastrocnemius (upper calf) stretch:
– Stand facing a wall with the affected foot stepped back, toes pointing forward
– Keep the back heel flat on the floor, back leg straight
– Bend your front knee until you feel a stretch in the back calf
– Hold 30–45 seconds, 3 repetitions, 2–3 times daily
Soleus (lower calf) stretch:
– Same position, but bend the back knee slightly while keeping the heel down
– You’ll feel the stretch lower and deeper in the calf
Strengthening: Heel Raises with Toe Extension
This is the cornerstone exercise for rebuilding the fascia:
1. Place a folded towel or book under your toes to raise them (this engages the windlass mechanism and loads the fascia appropriately)
2. Rise onto your heels slowly; hold briefly at the top
3. Lower down very slowly — the slow lowering is key
4. Aim for 5 sets of 10–12 repetitions every other day
5. As pain allows, progress to single-leg raises
Important: Some discomfort (4–5/10 pain) during this exercise is acceptable and expected. Sharp or severe pain means you’ve loaded too much — reduce the height or use both feet.
Footwear
- Avoid walking barefoot — especially on hard floors like tile or hardwood. The lack of arch support dramatically increases stress at the heel insertion
- Choose supportive footwear with a cushioned heel and moderate arch support the moment you get out of bed — keep a supportive pair of sandals or shoes at your bedside
- Rocker-bottom soled shoes (like certain HOKA or MBT styles) reduce forefoot and heel loading and can provide significant relief during recovery
- Orthotics — either prefabricated (available at most pharmacies) or custom-fitted by your physiotherapist — provide arch support and heel cushioning that offloads the fascia
Night Splints
If morning pain is severe, a posterior night splint maintains your ankle in a slightly dorsiflexed position while you sleep — keeping the plantar fascia gently stretched overnight instead of contracted. This can significantly reduce that first-step morning pain. Your physiotherapist can recommend the right type.
Ice
Apply an ice pack (wrapped in a cloth) to the heel for 15–20 minutes after exercise or after a long day on your feet. Frozen water bottles can double as a rolling massage — roll the arch of your foot over the bottle for 5 minutes.
Activity Modification
- Avoid sudden increases in activity — if you’re ramping up exercise, increase volume by no more than 10% per week
- Swap high-impact activities (treadmill running on hard surfaces) for lower-impact alternatives during recovery: swimming, cycling, or trail running on soft ground
- Monitor your 24-hour pain response — if activity causes pain that persists more than a few hours afterward, the load was too much
When to Seek Help: Warning Signs
Most heel pain is plantar fasciitis and will respond to the treatments described above. However, some symptoms suggest a different underlying cause that warrants prompt assessment.
See a healthcare provider promptly if you experience:
- Numbness, tingling, or pins-and-needles in the heel or along the arch — this may indicate nerve entrapment (such as Tarsal Tunnel Syndrome or Baxter’s nerve compression) rather than fascial pain
- Heel pain that wakes you from sleep or is worse at night — fascial pain is typically activity-related; night pain suggests nerve or vascular involvement
- Pain that is better with walking but worse with rest — standard plantar fasciitis worsens with weight-bearing; the reverse pattern can indicate nerve compression
- Swelling, redness, or warmth around the heel disproportionate to activity
- Fever accompanying heel pain — may indicate infection (osteomyelitis)
- Pain after a sudden trauma with inability to bear weight — this may be a calcaneal (heel bone) fracture
- Pain in children or adolescents — heel pain in young people is more likely to be Sever’s disease (growth plate irritation), a completely different condition requiring different management
- No improvement after 6–8 weeks of consistent conservative treatment — this warrants investigation to rule out stress fracture, inflammatory arthritis, or other pathology
A note on heel spurs: Many patients are alarmed when an X-ray shows a heel spur. It’s important to know that heel spurs do not cause plantar fasciitis. About 50% of people with plantar fasciitis have spurs, but so do many people with no pain at all. The spur is simply a sign of long-standing traction forces — treating the biomechanical cause of those forces is what resolves the pain, not addressing the spur itself.
Frequently Asked Questions
Will plantar fasciitis go away on its own?
Yes — it is a self-limiting condition, meaning it will eventually resolve. With no treatment, this can take 12–18 months or longer. With targeted conservative care, the majority of patients see significant improvement within 3–6 months and full resolution by 12 months.
Do I need to stop exercising completely?
No. Complete rest is rarely recommended and often counterproductive — it reduces the load on the fascia without building its capacity to tolerate load, meaning pain typically returns when you resume activity. The goal is load management: modify your activities to stay within a pain-tolerable range while progressively rebuilding strength. Low-impact alternatives (cycling, swimming) are excellent during recovery.
Why is the pain worst in the morning?
Overnight, the plantar fascia contracts to its shortest resting length. When you stand up, it is suddenly stretched from that shortened state, causing micro-tearing at the already-degenerated insertion point. Stretching before your first step “pre-loads” the fascia gradually and dramatically reduces this shock.
Are cortisone injections a good idea?
Cortisone injections can provide meaningful short-term pain relief — typically effective for up to four weeks. However, research consistently shows they have no significant effect on long-term healing or on the thickness/structure of the fascia. Multiple injections also carry a risk of fascia rupture. They are best used as a short-term bridge to allow rehabilitation to begin, not as a stand-alone treatment.
What is the difference between plantar fasciitis and a heel spur?
A heel spur is a bony growth that forms on the heel bone due to long-standing traction forces from the plantar fascia pulling at its attachment point. Heel spurs are present in roughly 50% of plantar fasciitis cases but are a consequence of the mechanical stress, not the cause of pain. Most people with heel spurs have no pain whatsoever.
How is plantar fasciitis diagnosed?
Diagnosis is typically clinical — a physiotherapist or physician can usually diagnose it from your history and a physical examination (location of tenderness, pain pattern, ankle dorsiflexion assessment). Imaging is rarely needed for initial diagnosis but may be ordered if symptoms are atypical, severe, or not responding to treatment, to rule out stress fracture, nerve issues, or other pathology.
Can plantar fasciitis come back after treatment?
Yes, it can recur — particularly if the underlying causes (calf tightness, biomechanical factors, footwear) are not addressed. This is why physiotherapy focuses not just on resolving current pain but on correcting the mechanics that caused it, and on building the foot strength to prevent recurrence.
When is surgery considered?
Surgery (typically an endoscopic plantar fasciotomy) is a last resort for chronic cases where all conservative treatments have been exhausted over a period of at least 12 months. It is rarely needed — the overwhelming majority of patients achieve full recovery without surgery.
Ready to Start Your Recovery?
If heel pain is disrupting your mornings, limiting your movement, or holding you back from the activities you love, our team at Wellness Place is here to help. We take an integrated approach — combining physiotherapy, shockwave therapy, acupuncture, and massage in a plan that is tailored to your specific situation.
You don’t have to accept this pain as part of your daily life. Most people with plantar fasciitis recover fully. Let’s get you there.
This article is intended as a patient education resource. It does not constitute medical advice. Please consult a qualified healthcare provider for assessment and treatment of your specific condition.