Pelvic Pain: Understanding a Complex Condition — and Finding Relief
What Is Chronic Pelvic Pain?
Chronic pelvic pain (CPP) is pain in the lower abdomen or pelvis lasting 6 months or more, not exclusively related to menstruation or intercourse. It affects approximately 15–25% of women and is one of the leading reasons for referral to gynaecology.
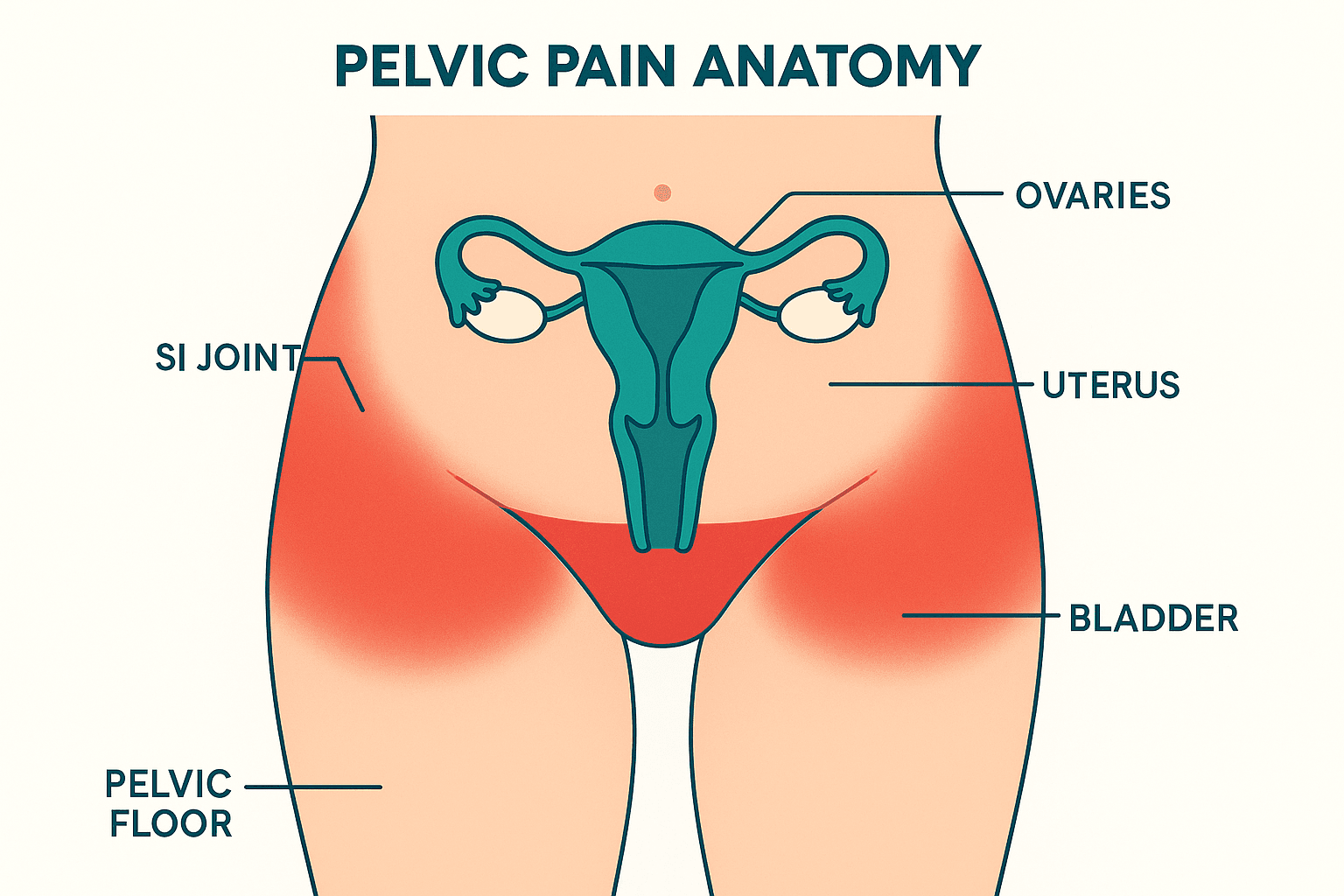
But CPP is rarely caused by a single structure. It typically involves a complex interplay of:
– Musculoskeletal factors — pelvic floor muscle dysfunction, sacroiliac joint irritation, lumbar spine involvement
– Visceral factors — bladder (interstitial cystitis), bowel (IBS), uterine/ovarian pathology
– Neurological factors — central sensitization, nerve entrapment
– Psychological factors — past trauma, anxiety, depression (which both contribute to and result from persistent pain)
Treatments at Wellness Place
Pelvic Floor Physiotherapy
Pelvic floor physiotherapy is central to the management of almost all pelvic pain with a musculoskeletal component.
Assessment: A comprehensive history (pain pattern, aggravating/relieving factors, cycle relationship, bowel/bladder symptoms, sexual function, psychological wellbeing) combined with pelvic floor assessment — with full informed consent — to map muscle tone, tender points, and trigger points.
Treatment for hypertonic pelvic floor:
– Manual therapy: gentle internal and external myofascial release of pelvic floor trigger points
– Progressive down-training: learning to consciously and fully release the pelvic floor muscles
– Breathing retraining: diaphragmatic breathing coordinates with pelvic floor relaxation
– Dilator therapy: for vaginismus and dyspareunia — graduated, self-directed desensitization
– Trigger point release: addressing pelvic floor trigger points that refer to the pelvis, thighs, and lower back
Whole-body assessment: The lumbar spine, sacroiliac joints, hips, and coccyx all contribute to pelvic pain. Your physiotherapist addresses the full musculoskeletal picture.
Pain education: Understanding the neurobiological mechanisms of pelvic pain — central sensitization, visceral-somatic convergence — reduces fear and improves treatment engagement.
Acupuncture
Acupuncture has meaningful evidence for pelvic pain management, particularly for:
– Endometriosis pain — multiple systematic reviews confirm acupuncture reduces endometriosis-associated pain, including dysmenorrhoea and chronic pelvic aching
– Dysmenorrhoea — primary menstrual pain responds well to acupuncture
– Generalized pelvic floor tension — systemic nervous system regulation, reduction of the stress response that perpetuates pelvic floor holding patterns
– Interstitial cystitis — bladder point protocols reduce urgency, frequency, and pain
For pelvic pain with a significant stress/anxiety component, acupuncture’s systemic calming effects are particularly valuable — many patients notice that pelvic tension is directly related to overall nervous system arousal, and acupuncture helps break that cycle.
Frequently Asked Questions
My pelvic pain gets worse with stress — is that normal?
Yes, and it is important to understand why. The pelvic floor is part of the stress response system — the body “holds” in the pelvis under psychological stress, just as it holds in the shoulders and jaw. This is a very common pattern, and one that acupuncture and nervous-system-aware physiotherapy directly addresses.
I’ve had negative gynaecological tests — why am I still in pain?
Many causes of pelvic pain — pelvic floor dysfunction, nerve sensitization, myofascial trigger points — do not appear on ultrasound, MRI, or laparoscopy. A normal scan does not mean there is no pain, and it does not mean there is nothing to treat. Pelvic floor physiotherapy is specifically designed to assess and treat the musculoskeletal and neuromuscular contributors that imaging cannot detect.
Is pain with sex always vaginismus?
Not always — painful sex (dyspareunia) can result from pelvic floor muscle tightness, insufficient lubrication, vulvar skin conditions, endometriosis, or interstitial cystitis, among others. Vaginismus specifically involves involuntary muscle spasm. Assessment by a pelvic floor physiotherapist is the most accurate way to identify the cause.
For patient education only. Not medical advice.